
Diagnosing Asthma in Children: A Guide for Parents
Why Is Diagnosing Asthma in Children So Difficult?
Asthma is the most common chronic lung disease in children. Yet despite how common it is, diagnosing asthma in children remains surprisingly tricky—and misdiagnosis happens frequently at all ages, but especially in younger children.
So why the confusion? First, many childhood conditions can look like asthma. A simple viral infection can cause wheezing that sounds exactly like an asthma attack. Second, children—especially those under five years old—often cannot perform standard breathing tests the way adults can. They may not understand the instructions or be able to follow them. And third, asthma symptoms in children can come and go. A child might wheeze for a few days, then be completely fine for months, leaving parents and doctors unsure whether asthma is truly the cause or just a passing respiratory infection.
Because of this, many experts now agree that asthma diagnosis should never rely on symptoms alone—objective testing is essential whenever possible. The good news is that by following a step-by-step approach using the right combination of tests, doctors can make an accurate diagnosis in the vast majority of cases.
The Two-Pillar Foundation of Diagnosis
For school-aged children (typically 5 years and older), the modern approach to diagnosing asthma rests on two essential pillars:
Pillar 1: A Suggestive History of Variable Respiratory Symptoms
The doctor will ask detailed questions about your child‘s breathing patterns. Key clues that point toward asthma include:
Wheezing — A whistling or squeaky sound, especially when breathing out
Nighttime symptoms — Cough, wheezing, or breathlessness that wakes the child up at night
Symptoms triggered by specific things — Exercise, cold air, laughing, crying, or exposure to allergens like pollen, dust mites, or pets
Symptoms that come and go — Days or weeks of normal breathing followed by episodes of trouble
Response to asthma treatment — Does a rescue inhaler make the symptoms better quickly?
Personal or family history — Does the child have allergies, eczema, or a parent with asthma? These are strong risk factors
Pillar 2: Objectively Confirming Variable Airflow Obstruction
This is where testing comes in. While the history can strongly suggest asthma, guidelines worldwide now recommend that objective testing should be performed to confirm the diagnosis before starting long-term treatment. Simply put: don‘t just listen to the story—measure the lungs.
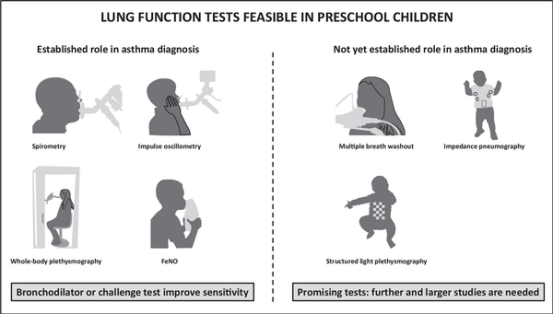
The Challenge of Diagnosing Preschool-Aged Children (Under 5 Years)
This is where diagnosis becomes genuinely difficult. Preschool children cannot reliably perform spirometry orFeNO testing, and there are no universally agreed-upon objective reference standards for this age group.
So how do doctors manage? They use a clinical approach based on four elements:
History of recurrent wheezing episodes — Has the child had repeated episodes of wheezing? And are episodes associated with specific asthma‑like triggers (viruses, exercise, laughing, allergen exposure)?
Exclusion of alternative diagnoses — Before labelling a young child with asthma, doctors must rule out other conditions that can cause wheezing in this age group. These include viral‑induced wheeze (very common and often not asthma), airway abnormalities like tracheomalacia (a floppy windpipe), foreign body aspiration, cystic fibrosis, and recurrent respiratory infections. Your doctor will take a careful history, examine your child, and may order additional investigations if these conditions are suspected.
A trial of treatment — For children under 5 with suspected asthma, many guidelines recommend starting a trial of daily low‑dose inhaled corticosteroids (ICS) for 8–12 weeks as a diagnostic test. If the child‘s symptoms improve significantly during treatment and worsen when treatment is stopped, that supports the diagnosis of asthma.
Response to a rescue bronchodilator — If your physician can actually listen to your child‘s chest during a symptomatic episode (in the clinic or emergency room), the response to a fast‑acting reliever inhaler can provide strong diagnostic clues.
Throughout this process, your child‘s doctor will review their progress regularly—every few months—and will attempt objective testing once your child turns 5 and can cooperate. If the diagnosis remains uncertain or the child’s asthma is poorly controlled despite treatment, an early referral to a paediatric respiratory specialist is strongly recommended.
Are Tests Always 100% Accurate? Understanding the Limits
No test is perfect. All diagnostic tests have two key statistical properties that doctors must consider:
Sensitivity — How good the test is at correctly identifying children who do have asthma (avoiding false negatives)
Specificity — How good the test is at correctly identifying children who do not have asthma (avoiding false positives)
Recent large studies of children aged 5–16 years have highlighted some important limitations:
FeNO at the 35 ppb threshold: sensitivity is modest—around 50–60%—meaning it will miss a significant number of children with asthma. However, its specificity is quite good (around 80–85%), meaning a high result is fairly reliable for confirming asthma.
Repeat FeNO testing: performing the test a second time increases overall diagnostic sensitivity by about 8% without reducing specificity—a useful strategy in borderline cases.
Spirometry: the sensitivity of bronchodilator reversibility is also modest, but its specificity when performed correctly is high.
House dust mite skin prick test: in one large cohort, the specificity was quite poor — about 62% — meaning roughly 2 out of 5 positive results may be false positives for asthma if used in isolation. This is why allergy testing should not be used alone to diagnose asthma.
The safest approach is to combine multiple tests rather than rely on any single test. A panel of FeNO, PEF variability, and allergy tests (IgE/eosinophil count) appears to offer the best practical combination of sensitivity and specificity.
Misdiagnosis: A Serious Problem
Misdiagnosis of asthma in children is common—both under‑diagnosis and over‑diagnosis occur frequently.
Under‑diagnosis means a child who actually has asthma goes undiagnosed and untreated. This can lead to unnecessary suffering—the child wheezes, misses school, cannot exercise—and an increased risk of severe asthma attacks. A study from Denmark showed that many children with unrecognised asthma simply do not report their symptoms to parents or doctors, partly because they have become accustomed to subtle breathlessness and do not realise something is wrong.
Over‑diagnosis means a child who does not actually have asthma is labelled as asthmatic and treated unnecessarily. A recent large study found that 53.5% of children initially diagnosed with asthma were considered over‑diagnosed after comprehensive objective testing. Over‑diagnosis leads to unnecessary medication use (with potential side effects and costs), a delay in finding the true cause of the child‘s respiratory symptoms, and unnecessary “sick role” labelling for the child and family.
The key message for parents: if your child has been diagnosed with asthma, it‘s reasonable to ask your doctor what objective evidence supports that diagnosis. For children aged 5 and above, if the diagnosis was made on symptoms alone with no spirometry or FeNO testing, you may wish to seek a confirmatory assessment.
What Parents Should Do
Be a good historian — Keep a diary: when does your child wheeze or cough? What seems to trigger it? Does it happen at night? After exercise? With laughter? Does a rescue inhaler help? These details are gold for the doctor.
Expect testing — If your child is 5 years or older and suspected of asthma, expect that your doctor will offer objective testing — FeNO, spirometry, or peak flow monitoring — before making the final diagnosis. If testing is not offered, you can ask why.
Don‘t panic if it’s not clear — Especially in preschool children, diagnosis can take time. A period of watchful waiting with a treatment trial may be perfectly appropriate. Your doctor should explain which pattern they suspect (viral wheeze versus atopic asthma) and how they will reassess over time.
Follow‑up matters — Whether diagnosis is confirmed or not, asthmatic children need regular review — every 4–6 weeks during initial treatment adjustment, then every 3–6 months once stable. This ensures the diagnosis remains correct and the treatment plan is working.
FIGURE 4 — A parent logging peak flow readings on a smartphone app
Regular monitoring of symptoms, triggers, and peak flow values helps track asthma control over time. The child‘s daily diary can be shared with the doctor at follow-up visits.
Description: A smartphone screen showing a ‘Paediatric Asthma Tracker’ app with morning and evening peak flow entries displayed as a line graph, with checkboxes for symptoms, triggers, and medications.
Image source: Asthma Self‑Monitoring for Children, American Academy of Allergy, Asthma & Immunology. Free use for educational purposes is permitted.
Quick Reference Guide for Parents
|
Question |
Answer |
|
What age can children start objective testing? |
Most children aged 5 and older can perform at least some tests (FeNO, spirometry, peak flow). Testing in children under 5 is generally clinical (history + treatment trial).-14 |
|
Which test is usually done first? |
FeNO (breath test). It‘s noninvasive, quick, and has reasonably good specificity. |
|
How do I prepare my child for testing? |
For FeNO + spirometry: avoid smoking (or vaping) in the home; do not give caffeine (e.g., cola, chocolate, tea) on the day of testing; the doctor may ask you to hold certain asthma medications for a specific time window beforehand (follow the instructions provided). |
|
What if the FeNO test is normal but the history is very suggestive? |
Then your doctor will proceed to spirometry with bronchodilator reversibility, and/or peak flow variability testing. Normal tests do not rule out asthma. |
|
Can a child outgrow asthma? |
Many children with viralinduced wheeze in the preschool years do outgrow their symptoms. However, persistent atopic asthma starting in early childhood may continue into adulthood. This still needs to be followed up over time. |
|
My child was diagnosed with asthma years ago but has no symptoms now. Do they still have asthma? |
Possibly not. Asthma can go into remission in children. However, symptoms can return. Your doctor may recommend repeating objective testing (e.g., spirometry, bronchial challenge) to determine whether a current diagnosis is still warranted. Do not stop medication without medical advice. |
Final Message
Diagnosing asthma in children is not always straightforward. Symptoms alone are not enough. But with the right combination of a careful medical history and objective testing—FeNO, spirometry, peak flow monitoring, and when needed, allergy testing—doctors can make an accurate diagnosis for the vast majority of school‑aged children.
For preschool children, the path is less clear. Your doctor may need to rely on clinical judgment, the pattern of symptoms, a trial of treatment, and careful follow‑up over time. That‘s okay—but you should always understand the reasoning and know what signs to watch for.
If you are concerned that your child’s breathing problems have not been fully investigated, or if the diagnosis remains uncertain, do not hesitate to ask for a second opinion or a referral to a paediatric respiratory specialist.
