
The Breath of Discovery: How a Simple Lung Test is Unlocking the Secrets of the "Quiet Zone"
Introduction: The Lung’s "Quiet Zone"
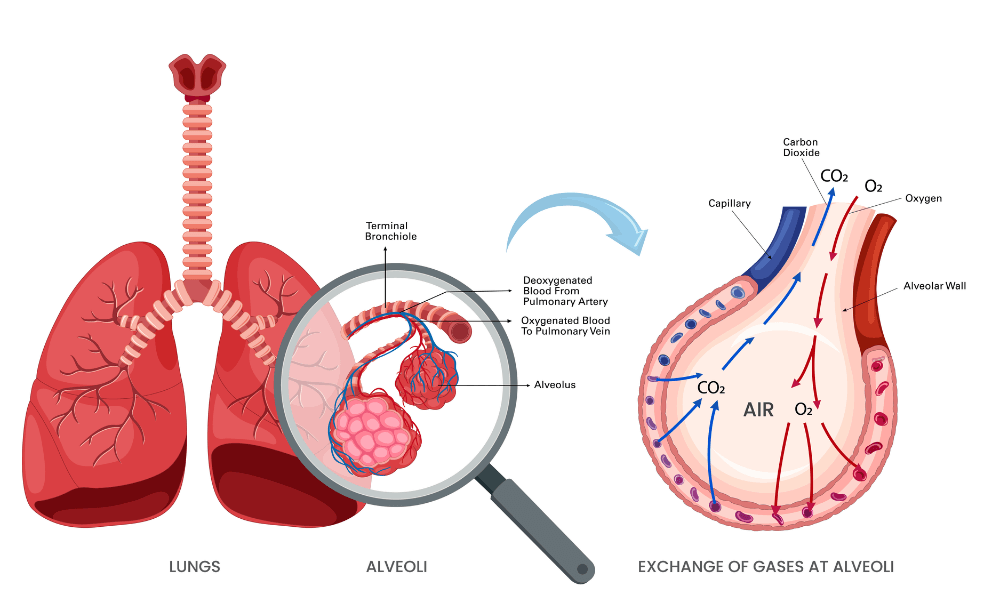
Imagine your lungs as a massive, upside-down tree. The trachea is the trunk, the bronchi are the large branches, and the bronchioles are the tiny twigs at the very end. For decades, when doctors wanted to check for inflammation in this tree, they focused on the "trunk" and the "large branches." These are the areas where wheezing is loud and obvious.
But there is a deeper region, the "quiet zone"—the small airways (less than 2 millimeters in diameter). These tiny twigs are the workhorses of oxygen exchange, but they are also the most vulnerable. They are the first to show signs of early disease and the most difficult to examine with standard breathing tests.
Enter CaNO—a revolutionary, non-invasive biomarker that is finally giving doctors a window into this forgotten territory.
What is CaNO?
CaNO stands for alveolar nitric oxide. To understand it, we must first understand FeNO (fractional exhaled nitric oxide), which is a standard test for large airway inflammation (like in classic asthma).
-
FeNO measures the nitric oxide released from the large airways. It is a good test for allergic airway inflammation.
-
CaNO measures the nitric oxide released from the very bottom of the lungs—the alveoli and the small airways.
Think of it like this: If your lungs were a factory, FeNO would measure the smog near the smokestack (the large pipes), while CaNO would measure the pollution at the production floor (the deep, small spaces). A high FeNO tells you the "pipes" are inflamed; a high CaNO tells you the "production floor" is inflamed.
How is CaNO Measured?
The beauty of CaNO is its simplicity. It is a breath test that takes about 10 minutes.
-
The patient breathes in deeply to empty the lungs of all ambient air.
-
They exhale slowly and steadily into a specialized device at a controlled flow rate (usually 50 mL/second).
-
Using mathematical models, the machine separates the nitric oxide coming from the large airways (FeNO) from the nitric oxide coming from the deep lung (CaNO).
It is completely painless, does not involve needles, and can be repeated frequently to track disease progression.
Why is CaNO a Game-Changer?
Here is where it gets exciting for patients and doctors alike. CaNO is proving to be a critical tool in diagnosing and managing several chronic conditions:
1. Unmasking "Silent" Asthma (Small Airway Asthma)
Not all asthma is wheezy. Many patients experience shortness of breath, chest tightness, or fatigue during exercise that standard asthma tests cannot detect. These patients often have inflammation only in the "quiet zone." CaNO can identify these patients who would otherwise be misdiagnosed with deconditioning or anxiety, allowing them to receive proper inhaled therapy.
2. Predicting Steroid Responsiveness
Inhaled corticosteroids (ICS) are the backbone of asthma treatment. However, not all patients respond to them. Research shows that patients with high CaNO levels are much more likely to respond to ICS therapy than those with normal CaNO. This means doctors can avoid prescribing ineffective steroids to patients whose inflammation is caused by other factors (like obesity or smoking).
3. Differentiating COPD Phenotypes
Chronic Obstructive Pulmonary Disease (COPD) is often caused by smoking and is notoriously hard to treat. CaNO helps doctors see if a COPD patient has an "asthma-like" (eosinophilic) inflammation pattern. If CaNO is high, these patients might benefit from inhaled steroids, whereas standard COPD treatments usually focus on bronchodilators. This leads to personalized medicine.
4. Early Warning System for Disease Progression
Perhaps most importantly, CaNO levels often rise before symptoms flare up. For patients with severe asthma, a rising CaNO is an early warning signal that a "flare-up" is imminent. Doctors can increase medication early, preventing hospitalizations.
The Science Behind the Breath
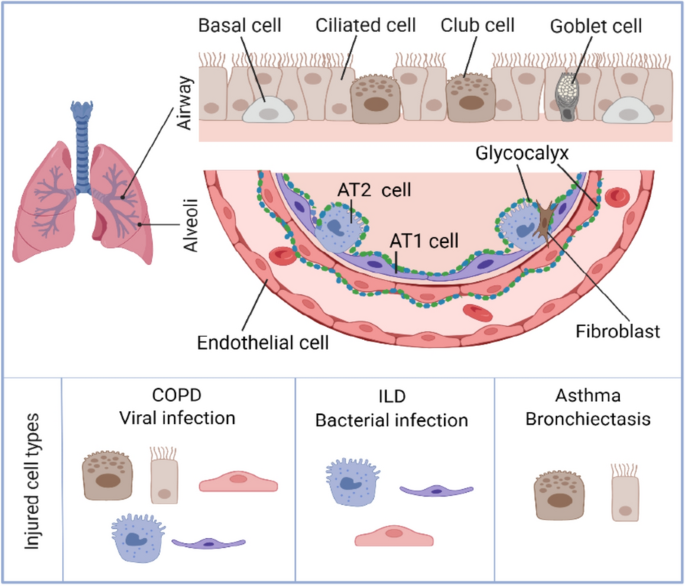
Why is nitric oxide high in these areas? It is because of a specific immune cell—the eosinophil—which releases the molecule IL-13. This molecule tells the lining of the airways to produce excessive amounts of nitric oxide. By measuring CaNO, we are essentially measuring the activity of these specific inflammatory cells deep in the lung tissue.
Limitations and the Future
While CaNO is powerful, it is not a standalone diagnostic tool. It must be interpreted alongside clinical history, spirometry (breathing force), and imaging. Furthermore, smoking can suppress nitric oxide, meaning a low CaNO in a smoker might actually represent severe underlying disease.
Currently, CaNO testing is primarily used in specialist respiratory clinics. However, as the technology becomes cheaper and more portable, it is likely to become a standard part of routine check-ups, much like blood pressure monitoring.
Conclusion: Listening to the Quiet
The small airways have been the "dark matter" of pulmonology—invisible, vital, and largely unmeasurable. CaNO technology has illuminated this space. For patients suffering from unexplained breathlessness, treatment-resistant asthma, or early-stage COPD, this simple breath test offers hope. It transforms a deep, invisible biological process into a number that doctors can use to tailor treatment. In the future of respiratory medicine, your breath will tell the whole story—from the trunk all the way down to the smallest twigs.

